The 2011 ASCO meeting ended last week. An estimated 20,000 physicians and others with research and clinical interests in cancer care attended. 4500 abstracts of scientific work were presented with tremendous publicity given to many of the studies, particularly those sponsored by pharmaceutical companies. Reporting on the “event” was obvious on financial pages, daily newspapers and the web.
Drugs and studies touted included the use of exemestane in breast cancer presentation, the use of vemurafenib in melanoma, use of pemetrexed maintenance, bevacizumab in ovarian cancer, targeted therapy, and so on. What was pointedly missing was any emphasis on costs or even mention of the relative cost effectiveness of the various regimens so vigorously publicized.
ASCO accepts a great deal of money from the pharmaceutical industry but even so, as a professional organization in a time when health care spending is soaring, one would think they would pay more than lip service to the problem.
ASCO’s lip service:
In the U.S. health care system, the challenge of coping with cancer, and the effect of both disease and treatment, can be compounded by the uncertainty of whether patients will have access to appropriate care and who will pay for it. It is clear that the costs of cancer care are going up, driven in large part by innovation and by our ability to do more for patients.
In many settings these costs are being shifted to our patients, with a poorly understood effect on access to care and treatment decisions. There is a clear need to better understand the financial effect of cancer care on our patients and how we as oncologists can best promote informed decision making and access to appropriate care.
And:
For decades, it has been clear that a lack of health insurance leads to patients with cancer presenting with more advanced stages of disease at the time of diagnosis and to worse outcomes. The recent passage of the 2010 Patient Protection and Affordable Care Act promises to reduce the ranks of the uninsured, currently estimated at more than 50 million people.
More than 25 million additional Americans may be considered “underinsured” based on inadequate coverage for medical expenses. Ideology aside, we likely can agree that all patients with cancer should have access to quality health care, and that guaranteed access to screening, timely diagnosis, treatment, and supportive care should be our priority for any emerging policy. At this time, there is a patchwork of services and support that can provide financial assistance for patients with cancer.
And:
Despite the availability of financial assistance programs, one-third of patients with cancer report trouble paying their bills and up to 25% report exhausting their savings. These figures are perhaps not surprising in light of the costs of treatment, particularly with novel molecularly targeted agents. Drugs that extend median survival by several months may be priced at as much as $100,000 per patient.
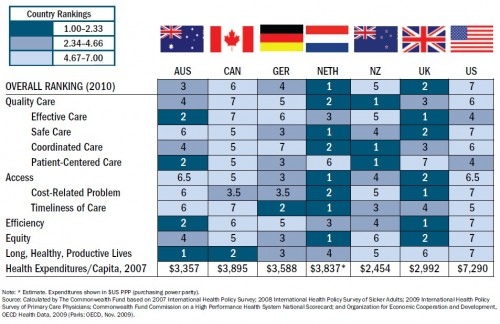
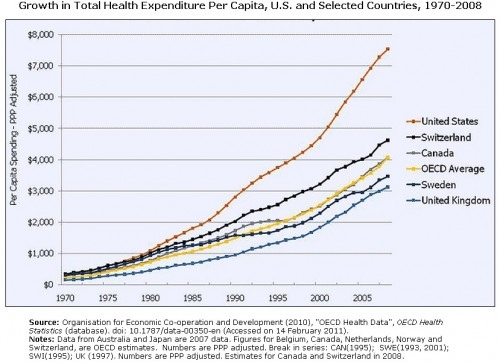
Costs are indeed a problem in our chaotic non-system of care. Where else in the industrialized world do you find 50 million uninsured and people bankrupted by health care costs. Only in America.
When searching the 4500 abstracts of presentations at ASCO 2011 for the word “cost” 286 (6.3% ) studies were found. On review most of these abstracts mention the word “cost” but do no analysis of the actual cost of the intervention.
When the 4500 abstracts were searched for the words “cost effectiveness” a mere 50 (1.1%) studies are highlighted. Once again the great majority of these don’t measure cost effectiveness. In the end fewer than 15 or less than .3% of all presentations were cost effectiveness analyses.
Part of the problem of course is funding. Drug companies are not interested in cost containment, cost efficiency, or value. Rather, their primary goal is ever increasing revenue and profits. They rarely fund cost effectiveness or comparative effectiveness studies unless they are trying to gain an edge over a competitor’s product. And if the study doesn’t show the company’s product positively, they are not publicized, presented or published.
Over the next couple of weeks I’ll review some of the studies of cost effectiveness and point out a few that PHarma did not tout during its publicity blitz last week.
If you are interested you can browse the 2011 abstracts yourself.