
I’ve previously talked about the manipulation of medical prices through price gouging and medical code game playing. What follows is an example. Not unusual. It happens every day in the U.S. of A.

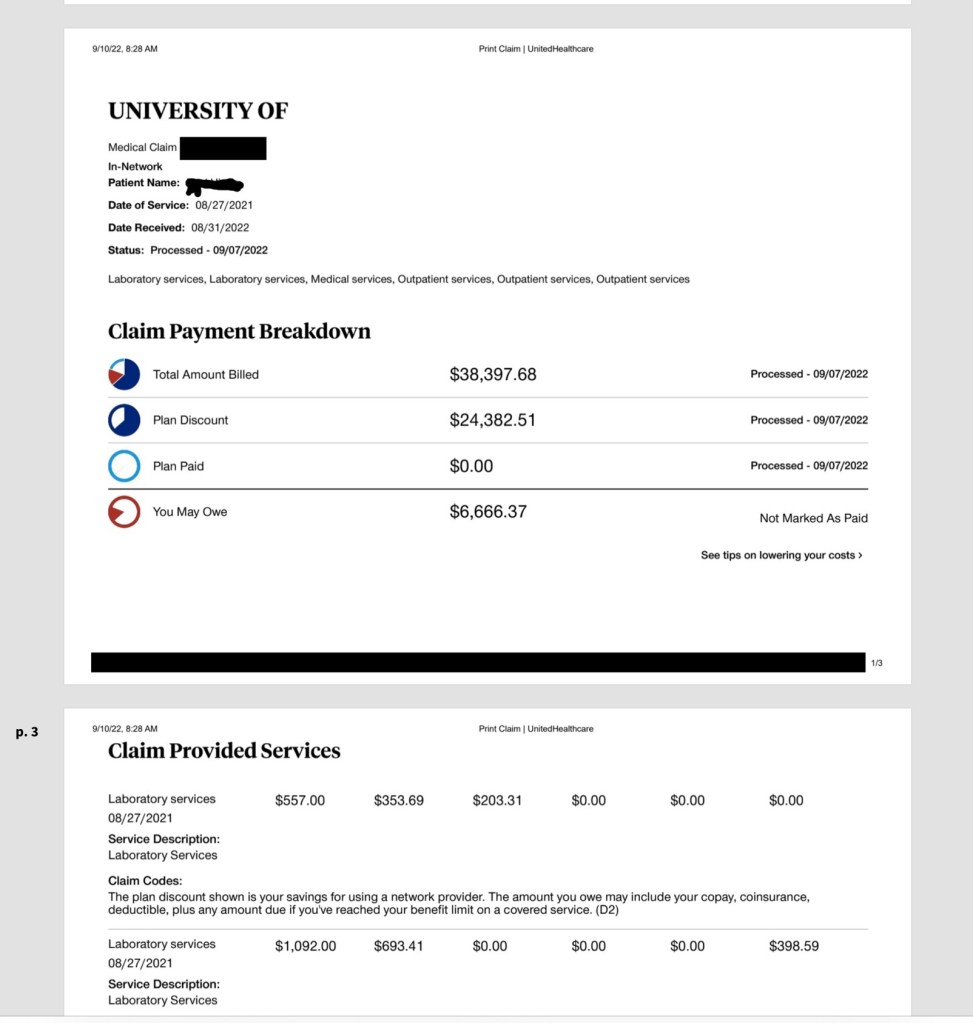
“Total Bill: $73,812 for the two shots ($35,414 for the first, $38,398 for the second), including lab work and physician charges. United Healthcare’s negotiated rate for the two shots plus associated fees was $27,568, of which the insurer paid $19,567. After Hinds haggled with the hospital and insurer for more than a year, his share of the bills was determined to be nearly $7,000.”
Medicynical Note: Almost everything on this bill is a manipulation of the system. First, the pricing of the lab tests. Each are inflated probably several times the actual cost of doing the test or the price of the test done for outpatients. Next, the cost of the medication leuprolide $35,000 (gasp!). This, for a drug developed in 1973 and priced at a few hundred dollar just a few years ago and costing $250 or less in overseas healthcare systems. Current pricing in various locales here. And lastly the use of codes to increase the billing i.e. separating the office visit fee from an “evaluation and management” fee. Both events, of course, happened simultaneously. Or consider the over $500 fee for a quick, less than a 1 minute, administration of a drug that has almost no immediate side effects. The nurse administering the drug didn’t even have to find a syringe to draw up the medication as it comes ready to go in a syringe.
Healthcare pricing has little to do with actual costs. This patient had insurance and paid a “negotiated” reduced but still excessive amount. But if he had no insurance he would have been billed and held accountable for the full amount, unless maybe he could claim poverty or was a skilled negotiator.
The finances of healthcare in the United States are worse than going to a used car lot and dickering for a car……and more expensive. When you understand that the CEOs’ of so-called health-care companies major concern is income not outcomes than you understand why we pay so much.
