“As a new year and presidential election approach, Americans face a worsening crisis: the affordability of healthcare. More Americans than ever, about 92%, now have health insurance – and simultaneously face enormous bills.”
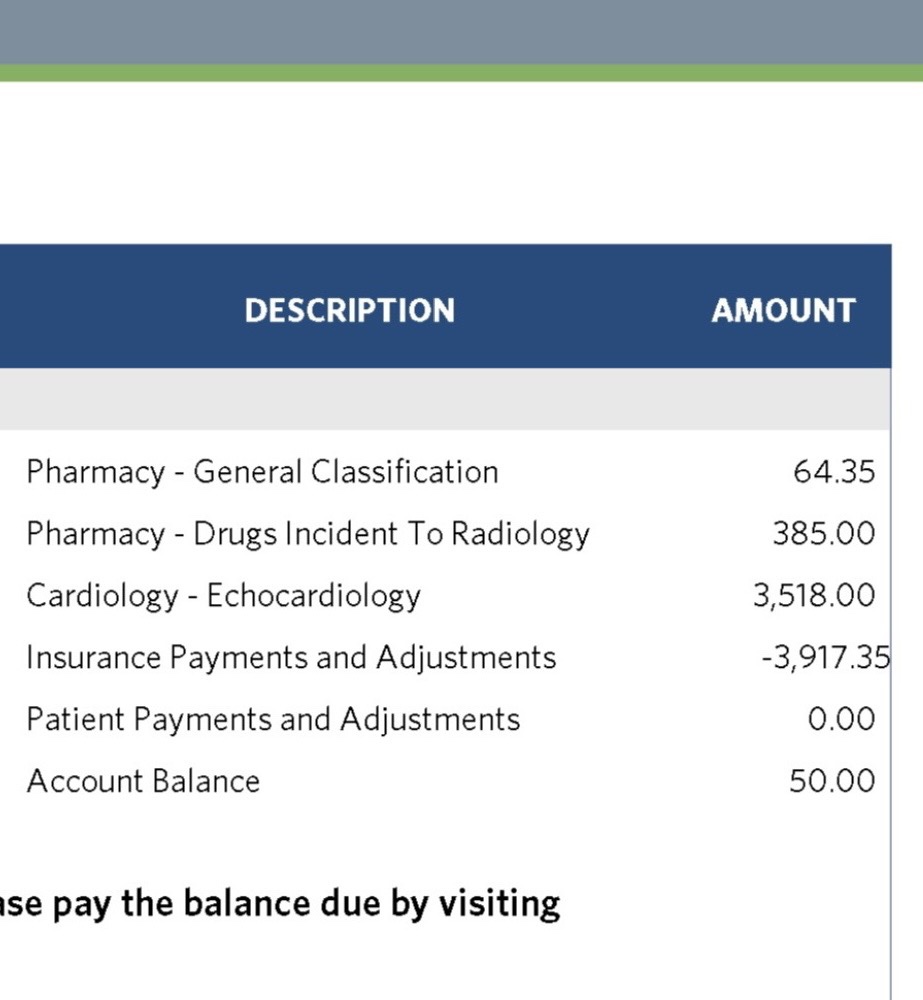
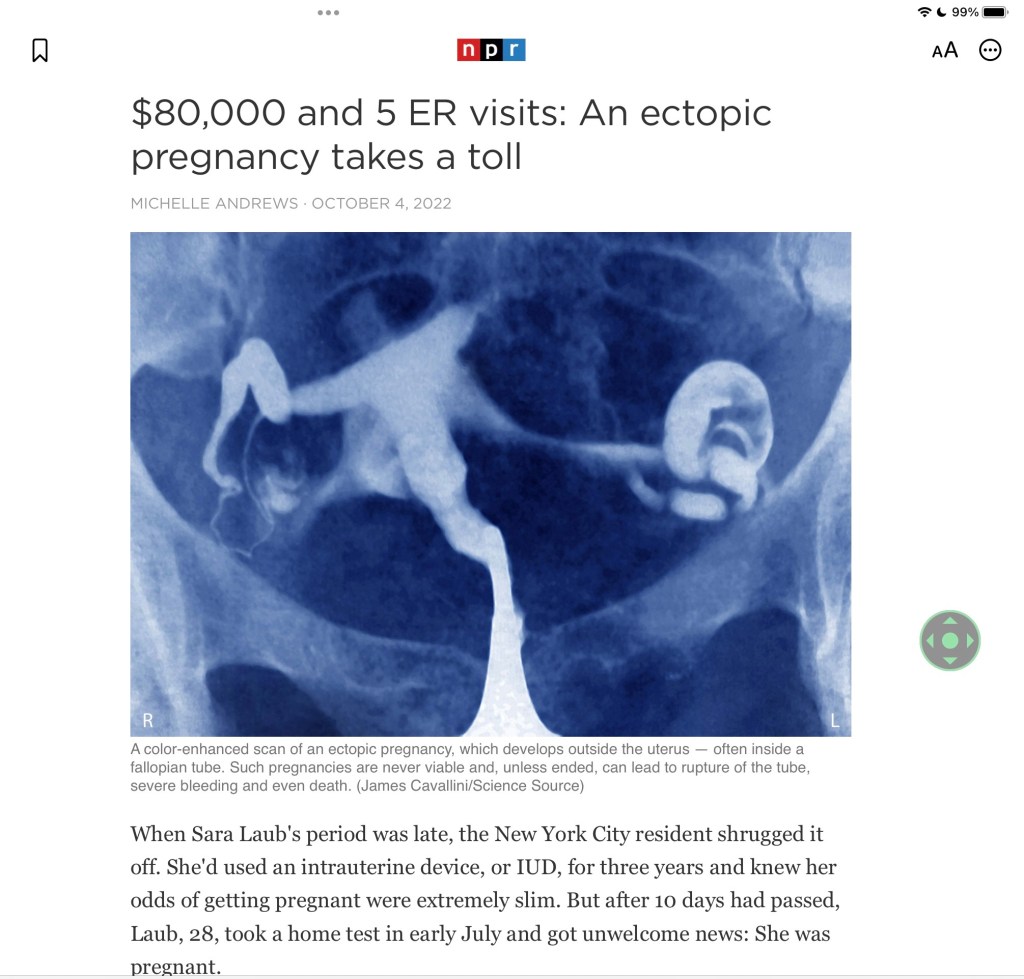
“Over the last decade, insurers and employers have pushed more cost-sharing onto individuals and families. Now, squeezed by medical costs and inflation, more than 100 million Americans have medical debt and roughly the same proportion report avoiding a prescription because of it.”

Medicynical Note: Americans pay more for healthcare, by a wide margin, than folks in any other industrialized nation. We pay more for doctor visits, hospital stays, medications, medical devices, insurance, everything.
We are also the only industrialized nation where there is medical debt. Why? It’s not rocket science. In a for-profit healthcare system everyone involved wants to make……. a profit.
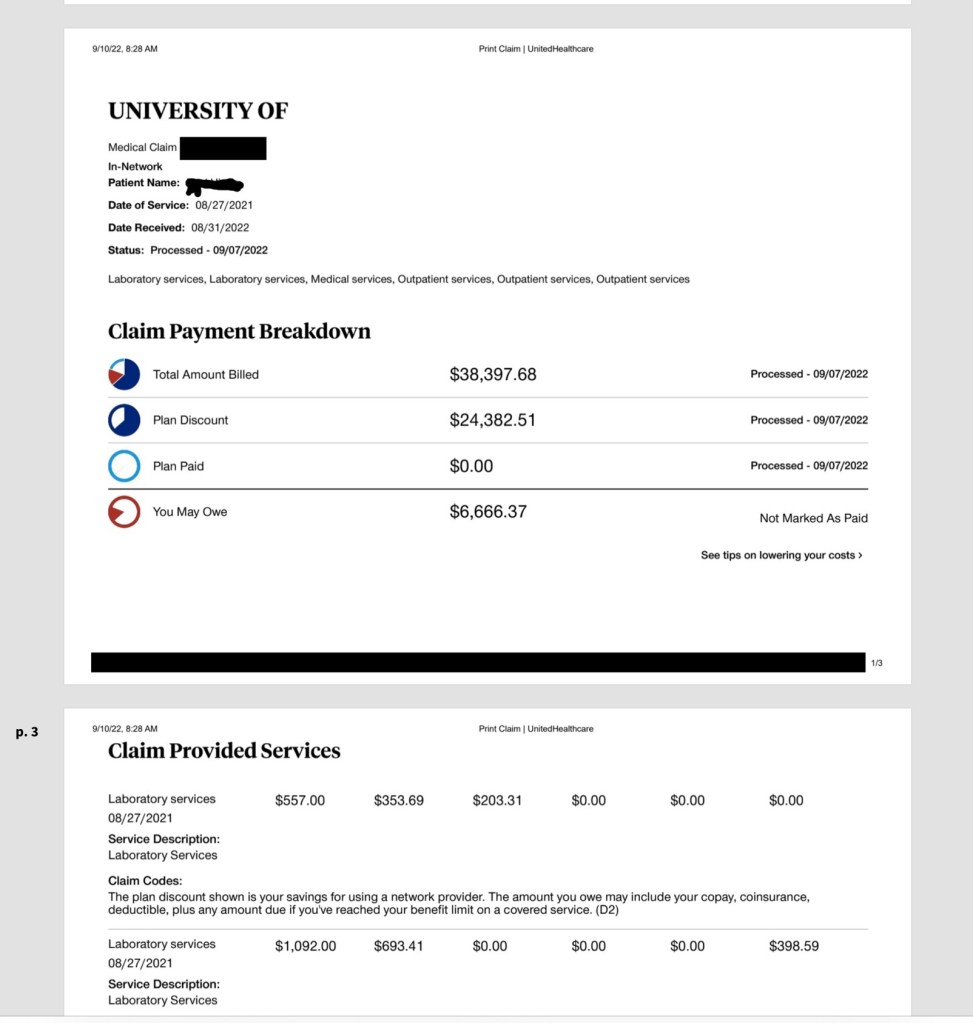
Why doesn’t the “marketplace” in our for-profit healthcare system work to control prices? Here, for a variety of reasons providers don’t have to compete on price, i.e. efficiency and value. And in any case, prices are not advertised or easily accessed. When you ask a hospital how much an operation or procedure will cost you will get a vague mostly inaccurate estimate or be told it “varies.” You literally can’t get an accurate total price for care. And lastly health care is not descretionary. When you really need it, you don’t have time, ability or motivation to shop for the “best” most economical option.
Adding insult to injury, one political party is planning make things worse and cut the already limited government supported health insurance programs if they win the next presidential election. They literally have no alternative plan for health care. Hint. That political party’s logo is an elephant.