This is from Economix–quoting Dr. David Cutler:
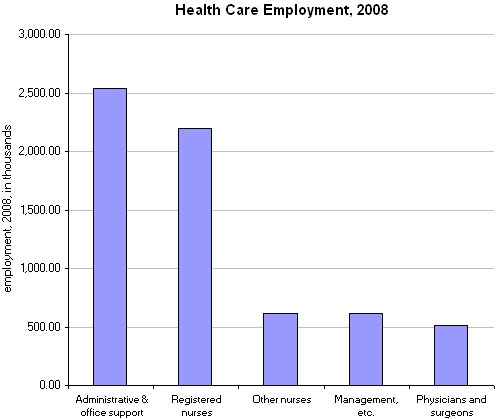
Medicynical Note: For every doctor there are 5, countem, five administrative and office support staff–and that doesn’t count another 500,000 “management” types. Guess who pays?

This is from Economix–quoting Dr. David Cutler:
Medicynical Note: For every doctor there are 5, countem, five administrative and office support staff–and that doesn’t count another 500,000 “management” types. Guess who pays?
Posted in General Cynicism, Health Economics
This from the New England Journal of Medicine in an article by Molly Cooke:
It is old news that the cost of medical care in the United States is unsupportable, yet we seem unable to grapple with the issue effectively. As current ideas for health care reform have percolated through Congress, cost-control mechanisms have generally been recognized as the weak component. Our country is remarkably generative in the development of new diagnostic tests, drugs, and procedures — and remarkably undisciplined in their deployment. New diagnostic and therapeutic procedures and the broadened application of established ones account for two thirds of the growth in health care expenditures.
Cooke believes medical schools and teaching institutions have a responsibility to teach cost consciousness in health care. Such a responsibility would seem natural given that health care is the largest expense of many people’s lifetime.
But:
Philosophically, we physicians have conceived of ourselves as, and taught students that we are, advocates for each patient, obligated to eschew all considerations other than benefit to that patient and his or her preferences.
And:
A predominant driver of the cost of hospital care is the length of stay, so a high priority is readying patients for discharge — which serves as a rationale for preemptively ordering any test and consultation that might be called for, to avoid delaying discharge. Consequently, students and residents have scarce opportunity to practice devising cost-effective diagnostic strategies and explaining their rationale to patients and families.
And
Finally, cultural values powerfully influence the selection of teaching topics. Academia celebrates the “high knowledge” of medicine: pathophysiology, molecular biology, genomics. Even evidence-based medicine, although it deemphasizes fundamental mechanisms, is regarded as acceptably intellectual in comparison with “low,” real-world concerns such as cost.
Medicynical Note: Teaching cost consciousness would apprear to be a no brainer given the near 17% of GDP spent on health care, the excessive costs of health care in the U.S. compared with elsewhere, the high medical related bankrupcy rate in our country, and our yearly excessive increase in health care costs. The article goes on to point out the urgent need to change and to value value!
Posted in General Cynicism, Health Economics
Jane Brody in today’s Times talks of the improvement in survival in multiple myeloma.
She notes there has been marked improvments in survival.
My guarded optimism stems from the progress made in devising treatments for several less well-known malignancies. For many patients with cancers like chronic lymphoma, chronic myelocytic leukemia and now multiple myeloma, longevity lies in the ability of science to remain one step ahead of the malignancy by unraveling its genetic and molecular underpinnings and producing treatments tailored to counter them.
How good is good?
The analyses found a definitive overall increase in the survival of MM patients over the past decade. In particular, five-year survival increased from 28.8 to 34.7 percent, and 10-year survival increased from 11.1 to 17.4 percent. Importantly, survival increased most dramatically in the youngest age group — more than half (56.7 percent) of patients younger than 50 survived at least five years, and more than 40 percent (41.3 percent) survived at least 10 years. In real years, the average relative survival increased from four years after diagnosis in 1990-1992 to almost seven years after diagnosis in 2002-2004.
Patients age 50-59 also fared well, with approximately half (48.2 percent) surviving at least five years, and nearly a third (28.6 percent) surviving at least 10 years. However, only modest increases were seen in the age group 60-69, and virtually no improvement was seen in patients older than 70. Since about half of MM patients are diagnosed when they are 60 or older, the lack of improvement in the eldest groups is a critical finding of the research.
Medicynical note: There are two problems with Brody’s analysis. First as noted in the latter review of progress there has been “modest” improvement for those age 60-69 and no improvement in patients older than 70. FYI the median age of myeloma patients is 66 with just 2%, thankfully, under age 40. Secondly, the cost of new treatments is excessive. The treatments recommended are in the range of $50,000-$100,000/year or more for the drugs alone and multiples of $100,000 for the transplants. This in a disease in which 5 year survival has “improved” to 34%.
Yes, there has been progress but it’s been mainly limited to younger patients and is at tremendous cost. We need to find a way to be more efficient and provide better value.
Pricing of health care in Massachusetts was analyzed by the Attorney General of that state. She found:
A. Prices paid by health insurers to hospitals and physician groups vary significantly within the same geographic area and amongst providers offering similar levels of service.
B. Price variations are not correlated to (1) quality of care, (2) the sickness of the population served or complexity of the services provided, (3) the extent to which a provider cares for a large portion of patients on Medicare or Medicaid, or (4) whether a provider is an academic teaching or research facility. Moreover, (5) price variations are not adequately explained by differences in hospital costs of delivering similar services at similar facilities.
C. Price variations are correlated to market leverage as measured by the relative market position of the hospital or provider group compared with other hospitals or provider groups within a geographic region or within a group of academic medical centers.
D. Variation in total medical expenses on a per member per month basis is not correlated to the methodology used to pay for health care, with total medical expenses sometimes higher for risk-sharing providers than for providers paid on a fee-for-service basis.
E. Price increases, not increases in utilization, caused most of the increases in health care costs during the past few years in Massachusetts.
F. Higher priced hospitals are gaining market share at the expense of lower priced hospitals, which are losing volume.
G. The commercial health care marketplace has been distorted by contracting practices that reinforce and perpetuate disparities in pricing.
Medicynical Note: Why do we pay more? Because our health care system is not a system. It’s a mechanism for manipulation and wealth accumulation not health care.
Posted in General Cynicism, Health Economics
Always thought patenting DNA sequences was the most outrageous abuse of the patent system, until drug companies charged more than the median and average income for a single drug.
Medicynic: It was as outrageous as the Supreme Court overturning a lower court to provide “free speech” rights to corportations by removing limits on campaign contributions. Hopefully they don’t overturn this!
Posted in General Cynicism
Costs continue to increase, this year we spent 17.3% of GDP on healthcare. But incomes are declining.
Medicynical Note: Those thinking our non-system is the best in the world should be informed that is isn’t and isn’t sustainable either. Hopefully health reform will affect the cost spiral–is it a bubble?
Posted in General Cynicism
 Medicynical Note: The opposition’s side show is quite amazing given these numbers. We certainly can’t continue like this. The party of NO has no ideas, no questions and no answers. Their views open the door to an empty room.
Medicynical Note: The opposition’s side show is quite amazing given these numbers. We certainly can’t continue like this. The party of NO has no ideas, no questions and no answers. Their views open the door to an empty room.
Passage of this bill is just a first step. Now comes the hard work and more decisions. We must now bring our costs in line with our competitors in the world. That will mean a careful look at expenditures; modifying our practice incentives; controlling the cost of innovation (patent reform) and controlling expectations–of patients, of providers and suppliers.
Posted in General Cynicism, Health Economics
For Dairy and other farmers who oppose health reform, is this socialism?
Dairy policy in the United states has been and is comprised of the following major components: (i) border measures that create import barriers for most dairy products and export subsidies for a few manufactured dairy products; (ii) government purchases of manufactured dairy products to support the farm price of milk.
Or this?
The U.S. Agricultural Department is required by law (various U.S. farm bills which are passed every few years) to subsidize over two dozen commodities. Between 1996 and 2002, an average of $16 billion/year was paid by programs authorized by various U.S. farm billsdating back to the Agricultural Adjustment Act of 1933, the Agricultural Act of 1949, and theCommodity Credit Corporation (created in 1933), among others.
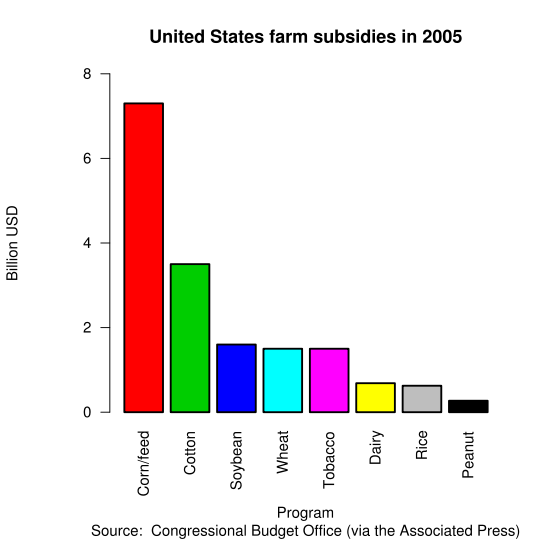
Medicynical Note: Medical care is bankrupting the country and individuals. We spend twice as much as other countries for care that is no better. As in agriculture, in medical care we need organization and regulation to assure affordable access. That’s not socialism it’s good government.
Posted in General Cynicism
Great apparent advance for some melanoma patients. A series in the NY times:
A new kind of cancer therapy, it was tailored to a particular genetic mutation that was driving the disease, and after six years of disappointments his faith in the promise of such a “targeted” approach finally seemed borne out. His collaborators at five other major cancer centers, melanoma clinicians who had tested dozens of potential therapies for their patients with no success, were equally elated.
Once unleashed, however, any cancer seemed to rely on the protein made by a particular mutated gene to fuel its wild growth. In all of the PLX patients, that gene was B-RAF. And whatever the cause, they came to consider themselves, so far as it was possible with what has always been a virtually untreatable cancer, charmed.
More here.
In new results from 31 melanoma patients with the BRAF mutation who were treated with 960mg of PLX4032 twice a day, 64% (14) of the 22 patients who could be evaluated so far met the official criteria for partial response (this involves the diameter of tumours shrinking by at least 30% for at least a month). A further six of the 22 patients also showed a response, but, at the time of the congress presentation, it was too early to say whether the tumours would shrink far enough to meet these criteria.
“What makes this treatment different from standard chemotherapy is that standard chemotherapy attacks the machinery involved in cell division; so to stop the cancer cells dividing uncontrollably, most standard chemotherapy aims to block the mechanism of division by interfering directly with DNA replication or with microtubules in the dividing cells. PLX4302 is different because it attacks the genetic programme that is causing the cells to divide uncontrollably, and we think the BRAF mutation is driving that programme. The drug is blocking the genetics of the tumour, rather than trying to interfere with the proliferation of the cells and, as a result, there are fewer side effects, although there are some. We are seeing some pretty dramatic and rapid responses, and they are occurring in sites where we rarely see responses to chemotherapy, such as in the bone.
Medicynical note: Until now melanoma has been refractory to virtually all interventions. This is a real positive step if the responses are durable and life extending–as they seem to be.
Posted in Cancer medicine (Oncology)
Health Insurance giant Anthem Blue Cross said it was raising rates on thousands of individual policyholders in California because the cost of their medical care exceeded the premiums they paid last year.
At the same time, other parts of Anthem reaped a profit. A Times analysis of the company’s regulatory filings shows that $525 million in Anthem’s earnings in 2009 was shipped to its corporate parent WellPoint Inc. The analysis was not disputed by Anthem.
Anthem Blue Cross has been so profitable that, since WellPoint acquired it in 2004, it has contributed more than $4.5 billion to the parent company’s bottom line.
Medicynical note: These hikes reveal the insurer’s strategy of segregating patients into risk groups. It allows Anthem to selectively raise rates on those who cost them more. So if you have a small group with a few patients with illnesses your rates will go up. If you are an individual buying health insurance you rates go up if you have illness, frequently to the point that you can’t afford the coverage. The rate hikes are designed to do just that.
Quite a system. Insurer’s can systematically extinguish their risk. Patients who need the coverage most are priced out of the market. They are forced to bankruptcy, government programs, and “free” ER use–the republican health plan.
Posted in General Cynicism, Health Economics
