One of the republican/conservative shibboleths is that we have the best health care system in the world. Medicynic has long noted the only thing systematic about our health care establishment is that it follows the money. We found this article with some blatant false conclusions: The World Should Catch Up With Our Health Care:
The article from Real Clear Politics notes:
- “Now it’s clear, as one example, that longevity is only partially connected to health care in the first place and that when you subtract homicides and accidents, we in America live longer than anyone, despite President Obama’s constant reiteration of the reform-encouraging and utterly deceptive thesis that we do not.”
Except that’s not true.

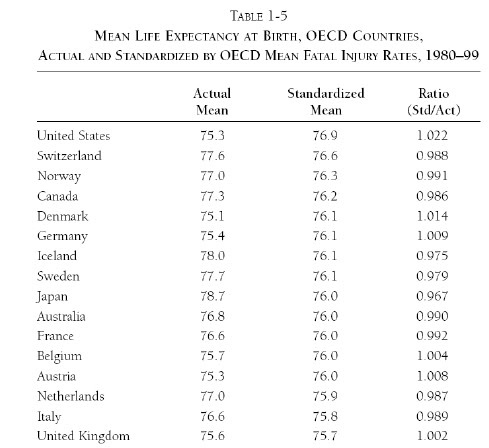
The author doesn’t tell on which data his broad statement is based but an AEI document makes this case here (http://www.aei.org/docLib/9780844742403.pdf) based on the above table. If indeed this is what his comments are based upon, the data is being misused.
The OECD has looked at the data on which this conclusion was based and it states: (See p. 20-21–“OECD Economic Surveys: United States 2008”, p. 1370)
“It has been claimed (Ohsfeld and Schneider, 2006) that adjusting for the higher death rate from accident or injury in the United States over 1980-99 than the OECD average would increase US life expectancy at birth from 18th of of 29 OECD countries to the highest. In fact, what the panel regression estimated by these authors shows is that predicted life expectancy at birth based on US GDP per capita (Medicynical observation: HEALTH SURVIVAL DATA FACTORING IN GDP IS NOT PURE SURVIVAL DATA, it’s skewed by the incorporation of income) and OECD average death rates from these causes is the highest in the OECD. The adjustment for the gap in injury death rates between the United States and OECD average alone only increases life expectancy at birth marginally, from 19th on average among 29 countries over 1980-99 to 17th. Hence, the high ranking of adjusted life expectancy mainly reflects high US GDP per capita, not the effects of unusually high death rates from accident and injury.”
Medicynic: in other words the data interpretation by Real Clear Politic is anything but clear–it’s flawed and the conclusion wrong.
- “We know that our treatments of serious disease produce better outcomes than elsewhere in the world, that everyone can get treatment at least in emergency rooms, that most Americans are satisfied with their care, that insurance net profits are a relatively low 3.3 percent and that the actual number of citizens without access to insurance is closer to 10 million than the 46 million number so often heard. We also know that Medicare and Medicaid have accumulated trillions of dollars in obligations to future recipients that we have no way of paying.”
Our outcomes of serious disease after diagnosis are indeed as good as elsewhere but at twice the cost. What other consumer good do we willingly buy at twice the price for the same product? Yet that’s what those opposing reform wish on us.
Regarding emergency room care. Our reliance on this has resulted in delays in care; diseases being treated at later stages than in other health care systems; it is by far the most costly inefficient care available;and is used when most problems could have been more economically treated. Guess who pays?
Use of ER care in place of assured regular access to care delays treatment and results in people dying for problems they might otherwise avoid. The following is from Commonwealth Fund, Health Affairs, World Health Organization
HOW THE US STACKS UP ON PREVENTABLE DEATHS
1. France — 65
2. Japan — 71
3. Australia — 71
4. Spain — 74
5. Italy — 74
6. Canada — 77
7. Norway — 80
8. Netherlands — 82
9. Sweden — 82
10. Greece –84
11. Austria — 84
12. Germany — 90
13. Finland — 93
14. New Zealand — 96
15. Denmark — 101
16. UK — 103
17. Ireland –103
18. Portugal –104
19. US — 110
The U.S. ranks at the bottom of 19 industrialized nations in the number of preventable deaths by conditions such as diabetes, epilepsy, stroke, influenza, ulcers, pneumonia, infant mortality and appendicitis. The number at the right represents the number of preventable deaths per 100,000 population in each country in 2002-2003.
That “most Americans are satisfied with their health care is probably true, since most Americans fortunately are healthy and a large number of these satisfied folks receive their coverage from the government, one way or another. What is also undeniable is that most Americans without such coverage and/or with significant illness are dissatisfied.
Medicynical Note: I don’t think the world in interested in inequity and inefficiency. The facts are we pay twice as much for health; have 50,000,000 uncovered by insurance; have no better and in many areas worse outcomes than other countries; and are being asked by our conservative brethren to accept this as the best we can do. 60% of bankruptcies have a medical bill component. In this, our (non) system is number 1.