The drugs Avastin (bevacizumab) and Provenge (sipuleucel-T) are two of the most expensive drugs in the world. Bevacizumab costs in the range of $100,000/year for treatment and simuleucel $93,000 for a course of treatment.
Neither cures patients. In studies in breast cancer bevacizumab has been found minimally effective, if at all. When compared to outcomes of patients not using the drug, It appears to delay progression by a few months and survival by even less then that (between no survival advantage to a few months). Sipuleucel-t gives about the same degree of response in prostate cancer. Despite this apparent lack of efficacy, and the advice of an FDA advisory board, Medicare has decided to continue to pay for the use of these agents.
The problems with these drugs are two-fold. One, they do very little to improve survival. And second, they are outrageously priced.
Regarding pricing, we’ve allowed drug companies to price drug grotesquely by:
- Providing them government sponsored monopoly (a patent) for a generation. (so much for free markets)
- Allowing drug companies to take drugs developed in part with government research funding private without offsetting the government’s investment by requiring licensing or reasonable pricing of the drug
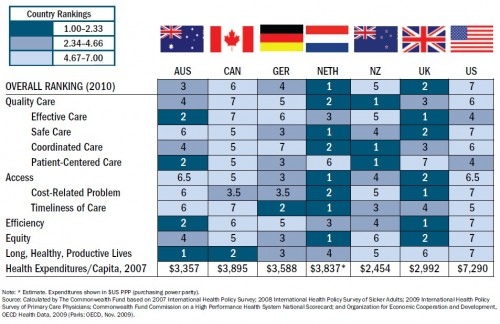
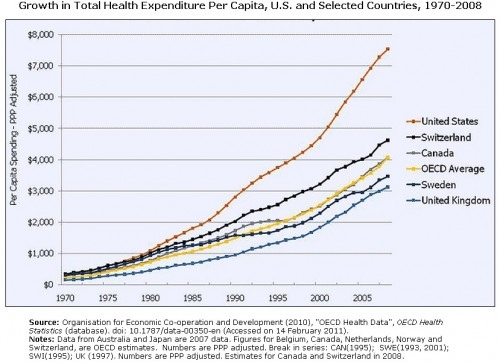
- Prohibiting Medicare from negotiating price with drug companies. This was part of the Medicare D law and has resulted in the inexorable upward spiraling of drug prices. We pay more for drugs in the U.S. than anywhere else in the world. WE ARE NUMBER 1!
- Cost effectiveness is not in our health care system’s vocabulary. We regularly use drugs with limited to no effectiveness.
Medicynical Note: For many years as an oncologist I used drugs with limited efficacy just on the chance that my patient might benefit. Desperate people accepted remarkable levels of toxicity in the hope that they will be the lucky ones and have a long survival benefit. During treatment, they all thought the drug was working, until it became clear that the disease was progressing. In retrospect very little of the “response” (and I’m thinking of patients with colon cancer treated with 5FU during the 70’s and 80’s) was tumor regression due to the drug. We almost never saw tumor’s decrease in size. Rather each cancer has a biology that affects how rapidly it will grow and recur. There are other poorly understood factors such as the patient’s immune system’s affect on tumor growth that also may come into play. But what was clear from comparison studies of 5 FU and no treatment was that very few patients benefitted. It should be noted that at the time 5FU in 500 mg vials cost $5.00.
Medicare has now announced that despite the proven limited efficacy of these drugs (bevacizumab and sipuleucel-T they will continue to pay for them–at the price demanded by the manufacturer.
If we are unable to rationally use these grotesquely expensive agents we will undoubtedly be rationing through increased co-pays, increased cost of insurance, and lo ball insurance that does’t cover such agents.