If you don’t believe we spend too much on health care check this out.
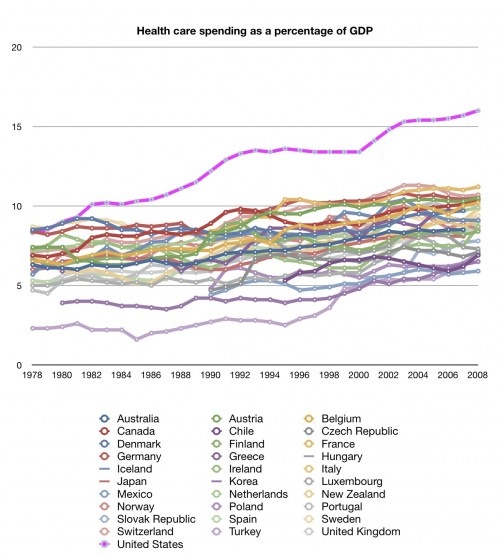


Medicynical Note: What’s most striking are the poverty rates: 14% overall, 17% for children, 22% for the elderly and income inequality. Our comparative expenditures on pre-primary education and finally the health rating of our population are also not very encouraging. Exceptional yes, but in the wrong way.
Posted in Ethics, General Cynicism, Health Economics
It’s difficult to believe anyone would want to deregulate control of drugs or for that matter medical devices. Without a neutral third party review of efficacy and safety, it’s anyone’s guess what would be foisted onto an unsuspecting public.
Consider that over the years defects have been very commonly found in such implantable devices. In fact thousands of recall notices/year are the norm.
Meanwhile, the number of items implanted in people’s bodies is soaring, as is the number of recalls. Nearly 2,500 medical devices were recalled for potential safety problems in fiscal 2008, according to the Food and Drug Administration. That was nearly double the number reported the previous year and a 164 percent increase since 2000.
With all this, we now have legislators who have accepted campaign contributions from venture capitalists working to undermine the oversight process:
Over the following month, Mr. Paulsen’s campaign committee took in $74,000 from people with a stake in device regulation, much of it from executives affiliated with venture capital funds and their spouses. Now Mr. Paulsen, a two-term Republican, is a sponsor of a bill that would make it easier to bring new medical products to market.
“They have this unwritten assumption that every new device is innovative,” Dr. Rita Redberg, who is the editor of the Archives of Internal Medicine, said, referring to the venture capital funds. But some devices, she said, “are killing people or causing significant harm.”
Further complicating the medical device business is the established fact that the gate keepers, medical providers, often take payment from device manufacturers to encourage use of their “innovations.” Without some brake in the system we have a recipe for development of faulty devices and their overuse and/or misuse.
Furthermore, these same forces want tort reform so as to protect these same manufacturers from being sued for bad outcomes from faults in the device and the selfsame overuse and misuse.
Note: Bringing devices to market without careful continuing oversight, when there is a money driven motivation, is a recipe for disaster.
Posted in General Cynicism, Health Economics
This, from CBS, says it all:
A dozen pharmaceutical companies have given doctors and other healthcare providers more than $760 million over the past two years – and those companies’ sales comprise 40 percent of the U.S. market.
With bucks that big flying around, is the quality of care offered by providers accepting them compromised? “Absolutely,” said Dr. John Santa, head of the Consumer Reports Health Ratings Center.
Medicynical Note: Guess who pays for this largesse? Is it any wonder that drugs in the U.S. cost 30% more than elsewhere in the world. Drug companies are uninterested in efficiency and value. It’s about the money. Sad but true.
Posted in General Cynicism, Health Economics
The Commonwatlth Fund’s review of U.S. health care provides assessments of our non-system’s efficiency, equity, access and quality.
Some good news can be found in an exception to the overall pattern of U.S. performance: rapid progress on quality metrics that have been the focus of national initiatives and public reporting efforts. Hospitals, nursing homes, and home health care agencies are showing marked improvement in patient treatment and outcomes for which data are collected and reported nationally on federal Web sites and as part of improvement campaigns. There has also been significant improvement in the control of high blood pressure, a measure that is publicly reported by health plans; increasingly, physician groups are being rewarded for improving their treatment of this and other chronic conditions. Better management of chronic diseases also has likely contributed to reductions in rates of avoidable hospitalizations for certain conditions, though rates continue to vary substantially across the country.
Of great concern, access to health care significantly eroded since 2006. As of 2010, more than 81 million working-age adults—44 percent of those ages 19 to 64—were uninsured during the year or underinsured, up from 61 million (35%) in 2003. Further, the U.S. failed to keep pace with gains in health outcomes achieved by the leading countries. The U.S. ranks last out of 16 industrialized countries on a measure of mortality amenable to medical care (deaths that might have been prevented with timely and effective care), with premature death rates that are 68 percent higher than in the best-performing countries. As many as 91,000 fewer people would die prematurely if the U.S. could achieve the leading country rate.
The summary also notes the cost burden and the lack of improvement in many health system indicators:
such as preventive care, adults and children with strong primary care connections, and hospital readmissions—likely stems from the nation’s weak primary care foundation and from inadequate care coordination and teamwork both across sites of care and between providers. These gaps highlight the need for a whole-system approach, in which performance is measured and providers are held accountable for performance across the continuum of care.
A nice chart shows some of the savings that would accrue if we actually had a system:

Medicynical Note: We spend more and have worse health care. Only in the U.S.
Posted in General Cynicism, Health Economics
Administrative costs in health care are a silent epidemic. Our inefficiency is costly to patients, providers, insurers, and government.
In many ways, our health care system mirrors our tax code — especially in its financing and health insurance facets. These can be made so complex and have been made so complex in the health care system in the United States that many decision makers in health care — patients, physicians, hospitals, employers and so on — need in-house or external consultants to find their way through the maze.
and:
Consulting firms help physicians bill private and public insurers or help patients submit claims to insurers after an illness. Legions of insurance brokers help prospective clients through the maze of the nongroup or small-group health insurance market. Large employee-benefit consulting firms, helping large companies, establish what amount, in effect, to analogues of the health-insurance exchanges in the Affordable Care Act, and many more consultants of many stripes are involved.
Medicynical Note: Yes the U.S. has the number 1 health care system in the world–it’s the most inefficient by far.
Posted in General Cynicism, Health Economics
The New England Journal of Medicine (NEJM) (Oct. 12, 2011) looks at the proposal to require drug companies to offer low income Medicare beneficiaries the same prices given Medicaid recipients:
Seems like a reasonable money saving idea but:
Reducing Part D payments for low-income beneficiaries, it is argued, could undermine incentives for the pharmaceutical industry to invest in research and development, as well as create illusory savings by shifting drug costs to other parties. In considering the wisdom of such deficit-reduction proposals, it’s important to consider how well the market is working for Part D and whether there are important inefficiencies that can be eliminated, resulting in budget savings.
It is pointed out however that the market doesn’t seem to work well with the indigent elderly who most often of the medicare group have multiple chronic conditions (30% of the group) and spends more on drugs than others in the medicare group.
It concluded that:
The approach obtains savings without undermining incentives for developing important new medical treatments. The anticipated side effects would be outweighed by the size of the estimated budget gains. This is as close to a win–win solution as we can get.
Medicynical Note: Put pressure on drug companies to offer more affordable drugs, why that may be Un-American. Consider that drug companies spend more on marketing than research; pay nothing to the government for drugs developed from government funded research; all have increased their prices and revenue by incredible amounts during a recession/depression.
Big PHarma will oppose this initiative preferring that we continue to pay more for drugs than any other industrialized country in the world. That’s really Un-American.
Posted in General Cynicism, Health Economics, Patents
The Washington Post notes the “hefty cost” of cancer treatment even for those with insurance.
Recent research spells out what patients are facing. A study by the Agency for Healthcare Research and Quality estimated that between 2001 and 2008, 13.4 percent of adults younger than 65 who had cancer spent more than 20 percent of their income on health care, including premiums. That compared with 9.7 percent of people with other chronic conditions and just 4.4 percent of those with no chronic conditions.
The article goes on to note the the increased bankruptcy rate among patients –over 6 times the baseline rate over 5 years.
ASCO the American Society of Clinical Oncology in the same article is noted to recommend :
The American Society of Clinical Oncology encourages oncologists to discuss treatment costs with patients. But that’s easier said than done, say some oncologists. More than half of the income of many oncology practices comes from administering the drugs they prescribe, says Ramsey, so oncologists are not entirely disinterested parties. In addition, the timing is often tough. Patients are “already scared and they have cancer,” he says.
Medicynical Note: It appears from their pricing of medications that drug companies have a sliding scale. The more life threatening the illness, the more the drug costs–whether or not it has a significant effect on the disease’s course
Another factor in the cost of cancer treatment, or any drug treatment purchased in the U.S., is that we pay more by 30%, for the exact same drug than other countries’ citizens. It’s a fact.
What’s amazing is that we tolerate the discriminatory behaviour of drug companies and pay the increased price.
The drug industry is lobbying furiously:
The primary trade group for the pharmaceutical industry spent $4.7 million in the second quarter lobbying the federal government on prices that federal health programs pay for prescription medicines and on other issues including patents, drug shortages and reimportation of drugs, according to a quarterly disclosure report.
And:
lobbied on implementation of aspects of the 2010 health care overhaul, including prices and rebates for drugs bought through the Medicare program, strengthening Medicare anti-fraud measures and eliminating an independent payment advisory board meant to hold down Medicare spending.
The article also highlights those former government officials currently lobbying their former colleagues on this issue.
Medicynical Note: Read the article. PhRMA opposes anything that will decrease drug prices. Consumer interest, value, access to less expensive drugs all are opposed by this group.
Since our esteemed Supreme Court ruled that corporations are citizens with equal rights to individuals, it appears that George Orwell’s truism from Animal farm has finally come to fruition. “All animals are equal but some are more equal than others.”
Posted in Ethics, General Cynicism, Health Economics
Interesting Economix by Uwe Reinhardt on money flow in health care:
He notes:
In fairness, it must be added that traditional Medicare basically sets prices and then just pays bills. It makes no active attempt to manage care (utilization controls, disease management, coordinating care and so on), because it has not been allowed by Congress to do so. It is almost as if Congress did not want traditional Medicare to be a prudent purchaser of heath care for the elderly. (Medicynical emphasis)
From the viewpoint of prudent purchasing, most economists would probably judge these prices too low. On the other hand, the fact that traditional Medicare just pays bills more or less passively may be precisely the reason that it is still so popular among the elderly. Traditional Medicare still offers beneficiaries completely free choice of providers and therapy — a degree of freedom that many younger Americans in insurance plans with limited networks of providers no longer enjoy.
Medicynical Note: Until we approach the issue of value in medicine (What works? Bang for the buck?) we’ll have the most expensive least efficient health care non-system in the world. What’s bugging us, the US, now is how to get to such a system.
Is health care part of the package of being a US citizen? Providing Medicare to the elderly and many with chronic illness implies such a commitment. Does required access to ER care for all, whether they can pay or not, point to a civic responsibility to assure access to care to the rest of the population?
If our republican friends really believe that health care is not a “right” then a large swath of citizenry are going to be in trouble as republicans follow through on this philosophy. Interestingly these rightist purists for some reason tout ER access for all as adequate health care in our non-system. Why they would choose the most expensive, least efficient care in the world as their means of providing health care is unknown.
If there is an explicit right to health care in our country, more efficient ways to provide it must be found. It should assure affordable care to citizens, including the elderly and those with illnesses. One problem has been that private insurers, ironically, want little to do with either of those populations.
Posted in General Cynicism, Health Economics
