
The following is from the CBO’s analysis of our economic future. (June 2009)
Holding down the spiraling levels of debt projected under either scenario could therefore result in significant economic benefits. However, accomplishing that goal would require some combination of substantial revenue increases and substantial spending decreases relative to current law. Those changes would have their own economic and social costs.
One policy that would prevent the increase in debt would be to raise revenues in line with the projected rise in spending. As evidenced by the estimated fiscal gap, the required increase in revenues under that approach would be large. If the increase occurred through higher marginal tax rates, incentives to work and save would be reduced and economic growth would slow.
An alternative policy would be to hold the growth of spending in line with the growth of the economy. That approach would require significant changes in the Medicare and Medicaid programs. Many experts believe that a substantial share of spending on health care contributes little, if anything, to the overall health of the nation, so changes in government policy have the potential to yield large reductions in federal spending without harming health. However, translating that potential into reality would require tough choices. It would ultimately depend on policymakers’ willingness to put ongoing pressure on the health sector to achieve efficiencies in the delivery of health care.
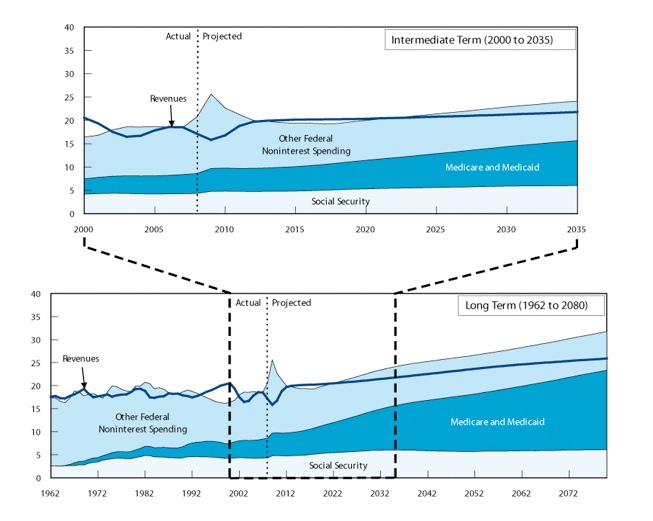
Reducing other federal spending significantly below the baseline levels would be difficult as well. Spending on Social Security has risen from almost 4 percent of GDP in the 1970s to almost 5 percent today and will increase to 6 percent in 2035 as the baby boomers retire. Other non-health, non-interest spending averaged almost 14 percent of GDP in the 1970s but has shrunk to about 10 percent of GDP over the past 15 years—aside from the current burst of spending in response to the recession and the financial crisis. Such spending is projected to decline further over time in CBO’s 10-year baseline.
Fine discussion by Brad de Long, (inflation economics lecture) of economic history, current high deficits and the decisions we face in meeting our economic commitments– and sustaining our health care non-system. The decisions and alternatives are enlightening.
He asks what we should do about it?
What do people think is the most likely outcome from this situation?
1. Come 2060 will we have raised taxes by a lot? We could double income taxes between now and 2060 and barely pay for extra government health spending.
2. Will we have cut doctors’ wages and enslaved them by drafting them into a socialist national health service?
3. Will we have abandoned our egalitarian healthcare beliefs?
4. Will the healthcare efficiency cost-effectiveness fairy have come and rescued us?
5. Or will the federal government as we know it will have collapsed and those of us who are still alive be involuntarily starring in a remake of Mad Max: Beyond Thunderdome?
Medicynical Note: Our non-system is not designed to deliver optimal care to our population but rather to provide excess profits to providers, suppliers and insurers. Over the years oversight, fiscal responsibility, efficiency and value have been degraded to the point of nonexistence. We therefore spend twice as much as most other places in the world; have reasonably good outcomes for those with access to care but mediocre population statistics (overall length of life, childhood statistics, prevention of preventable diseases, etc) presumably influenced by the 50 million people without insurance and those with limited access through such programs as Medicaid. We’re paying more but getting less benefit, this in the country that once fancied itself as the most productive and presumably efficient in the world.
We can continue to delude ourselves that we are the best in the world (as some radio hosts and 1/2 term governors do) or face reality that we are on an unsustainable path and do something.
