A flawed analysis of cancer costs appeared yesterday in numerous outlets:
It found that cancer treatment costs rose from nearly $25 billion in 1987 to more than $48 billion by the end of 2005. Medicynical note: Remarkably outdated information since the ACS is reporting expenditures of $93 billion in 2009. With indirect costs of an additional $18.8 billion. Which means a doubling or more of costs since 2005.
Better and more advanced treatments mean more people with cancer are remaining alive, so the spending increases represent money well spent, said Kenneth Thorpe, a health policy researcher at Emory University who has focused on the cost of health care.
“It seems like we’re buying increases in survival,” Thorpe said. Medicynical Note: I think most of the survival gain has to do with diagnosing cancer earlier (lead time bias) and/or changes in definition such that inherently more benign tumors are now lumped with cancer? (DCIS, Gleasons 5 prostate cancer for example).
The analysis of costs in this study stopped in 2005. In the last 5 years (since 2005) costs for cancer care have shown a remarkable acceleration associated with a decrease in those insured and a decrease in the quality of insurance. The data in this study is historical and probably not fully relevant.
As noted in the article.
Recent government reports have found that the percentage of Americans with private health insurance has been shrinking and recently hit its lowest mark in 50 years. Yet the study found that the proportion of cancer treatment costs paid by private insurance rose.
And companies have been tightening or cutting employee benefits, causing out-of-pocket costs to go up for many patients. Yet the study found that the proportion of bills paid by patients declined.
He alluded to widely reported increases in personal bankruptcies prompted by medical bills. “There’s no question that the out-of-pocket costs for some patients have risen dramatically,” Lichtenfeld said.
The study did not add in the cost of diagnostic tests and scans, which are cost drivers. And the data does not include the last five years, which saw some extremely pricey cancer drugs come on the market. Medicynical note: A PET scan costs in the range of $5000, more than the entire treatment course of the 1970’s.
Medicynical Note: Why publish this out of date analysis now?
This study might have been relevant 5 or 6 years ago, but it’s been overtaken by events. Health costs for cancer doubled between 1987 and 2005 (the period studied) AND remarkably have doubled again (see ACS data cited above) between 2005 and the present.
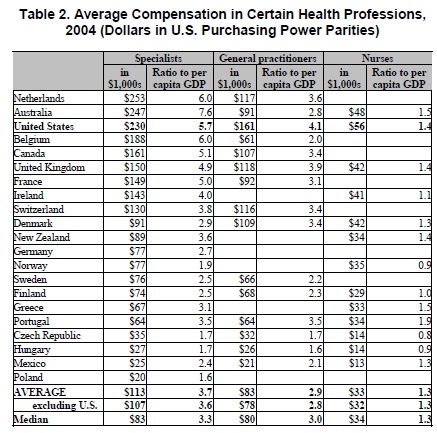
Meanwhile median and average salaries in the US declined in the last 10 years. Amazing and sobering.